From genotype to phenotype
Wolf-Hirschhorn syndrome with partial trisomy of 1q
ABSTRACT
A second-time gravida reported for evaluation of foetal congenital anomalies. Gestational age calculated by last menstrual period was 22 weeks and 2 days. The foetus was found to have multiple congenital anomalies during the anomaly scan and was subjected to medical termination of pregnancy. Maternal past history of full-term normal delivery with a healthy baby, now 5 years old. No history of systemic hypertension/pregnancy-induced hypertension or diabetes mellitus type 2 or gestational diabetes mellitus.Final diagnosis after medical termination of pregnancy and chromosomal microarray of the foetal parts turned out to be a case of Wolf-Hirschhorn syndrome (WHS) with partial trisomy of 1q secondary to deletion-duplication syndrome. A deletion-duplication syndrome, with a ~24.2 MB deletion on chromosome 4 and ~ 17.2 MB duplication on chromosome 1, suggesting translocation was noted.
INTRODUCTION
A second-time gravida reported for evaluation of foetal congenital anomalies. Gestational age calculated by last menstrual period was 22 weeks and 2 days. The foetus was found to have multiple congenital anomalies during the anomaly scan and was subjected to medical termination of pregnancy. Maternal past history of full-term normal delivery with a healthy baby, now 5 years old. No history of systemic hypertension/pregnancy-induced hypertension or diabetes mellitus type 2 or gestational diabetes mellitus.Final diagnosis:Chromosomal microarray of the foetal parts was done after medical termination of pregnancy.A case of Wolf-Hirschhorn syndrome (WHS) with partial trisomy of 1q secondary to deletion-duplication syndrome. A deletion-duplication syndrome, with a ~24.2 MB deletion on chromosome 4 and ~ 17.2 MB duplication on chromosome 1, suggesting translocation.a. distal deletions of the short arm of chromosome 4, including 4p16.3 micro-deletion syndrome, causes Wolf-Hirschhorn syndrome. The size of the deletion varies among affected individuals; studies suggest that larger deletions tend to result in more severe intellectual disability and physical abnormalities than smaller deletions 1,2.b. partial duplication on the distal region of the long arm of chromosome 1 is a very rare condition referred to as either pure trisomy or unbalanced translocations, affecting only 200 or so patients worldwide 3.
CASE REPORT
The fetus in this case had many features of both syndromes.i. congenital anomalies associated with WHS, that were noted in this foetus are: Prenatal growth retardation (IUGR), facial deformities (Greek warrior helmet appearance: high forehead, prominent glabella, hypertelorism, high-arched eyebrows, protruding eyes and micrognathia), cardiac anomalies- pulmonary isomerism, abnormality of the external ear 1,2.ii. congenital anomalies associated with partial trisomy of chromosome 1, that were noted in this foetus are protruding forehead and micrognathia.The prognosis of Wolf-Hirschhorn syndrome is poor. Frequently, this diagnosis is associated with fetal demise or infant death within the first year of life. Individuals who live past the first year of life, have a slow, but constant physical and mental development. About 1/3 of the patients die within the first two years of life due to a heart defect, aspiration pneumonia, or from a seizure. Only symptomatic treatment is available 1,2.Differential diagnoses: 1. Pitt-Rogers-Danks syndrome: has features that overlap with those of Wolf-Hirschhorn syndrome. Researchers now recognise that these two conditions are actually part of a single syndrome with variable signs and symptoms 2. In a foetus with multiple congenital anomalies, other trisomy syndromes such as trisomy 18,13 and 21 also merit consideration
DISCUSSION
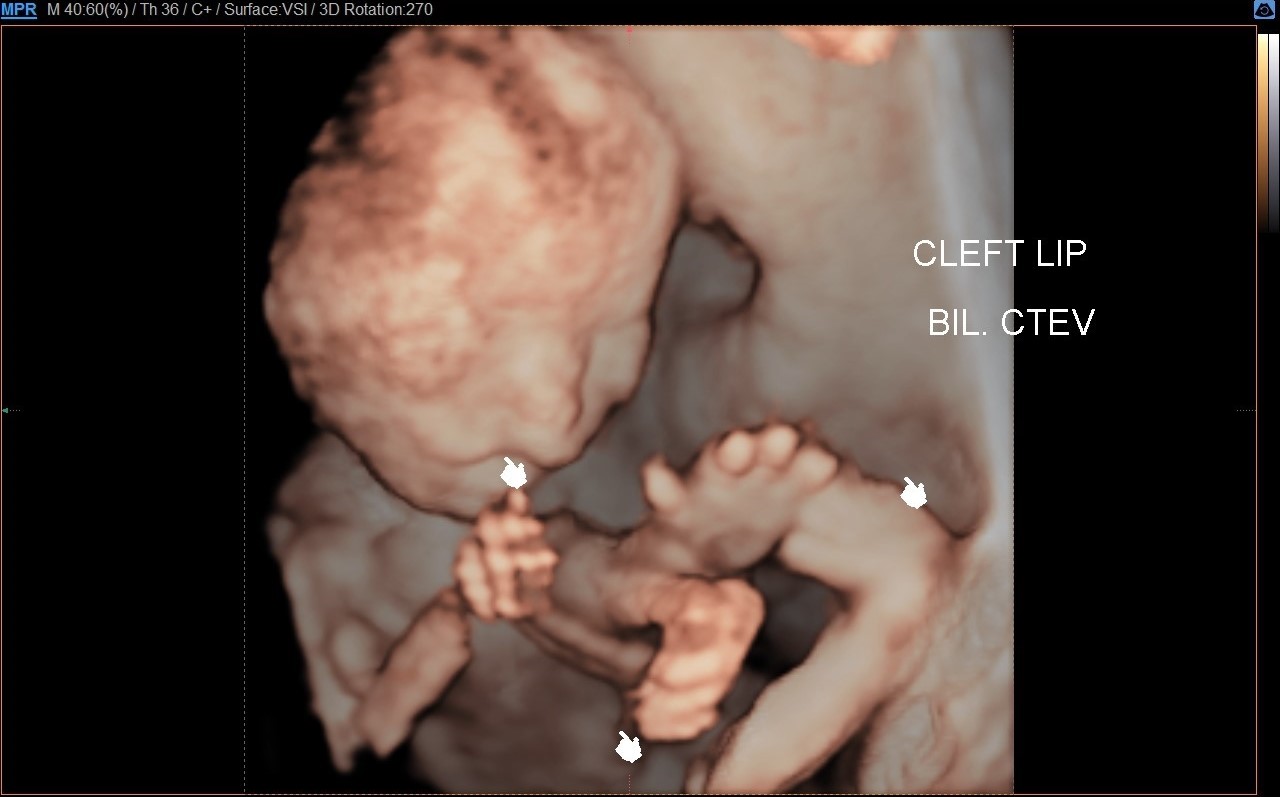
1. Reconstructed 3D image of foetal face and limbs shows evidence of unilateral right cleft lip, retrognathia/ micrognathia and bilateral congenital talipes equinovarus deformities.
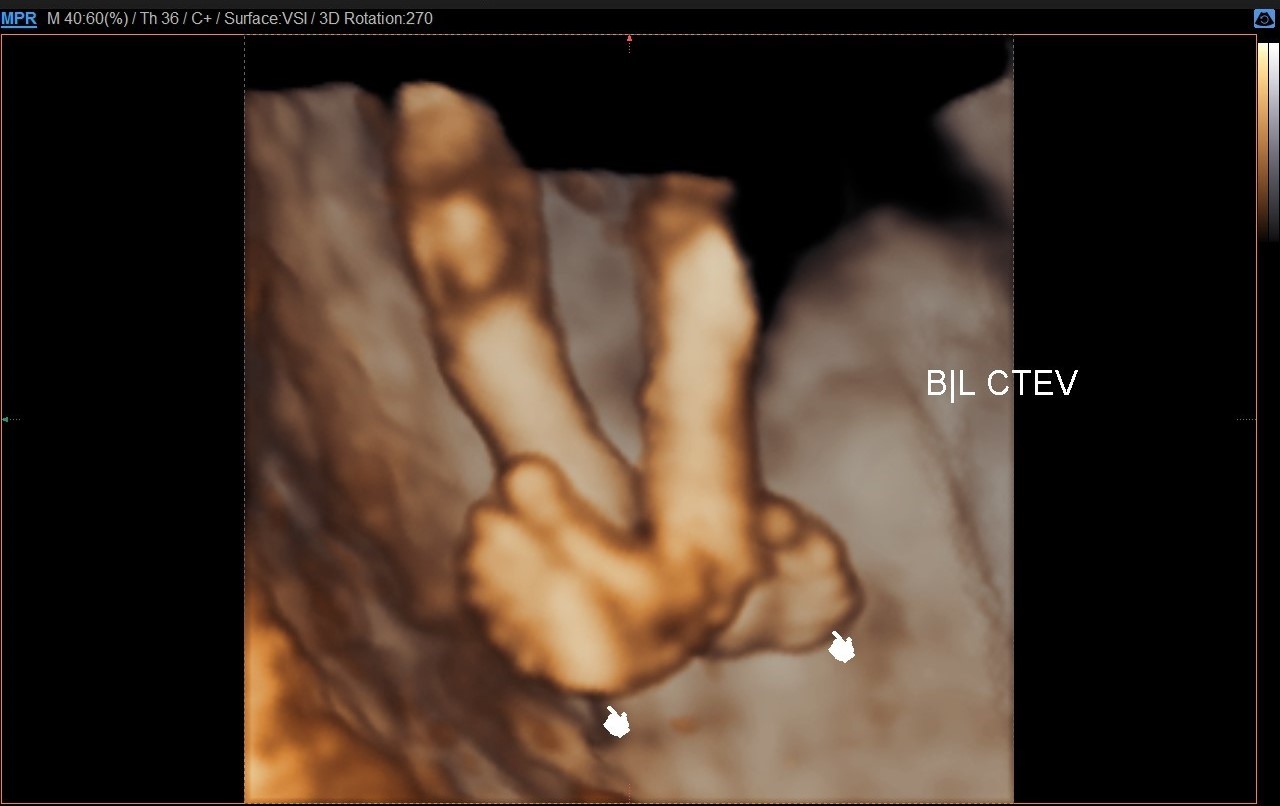
2. Reconstructed 3D image of the foetal legs shows evidence of bilateral congenital talipes equinovarus deformities.
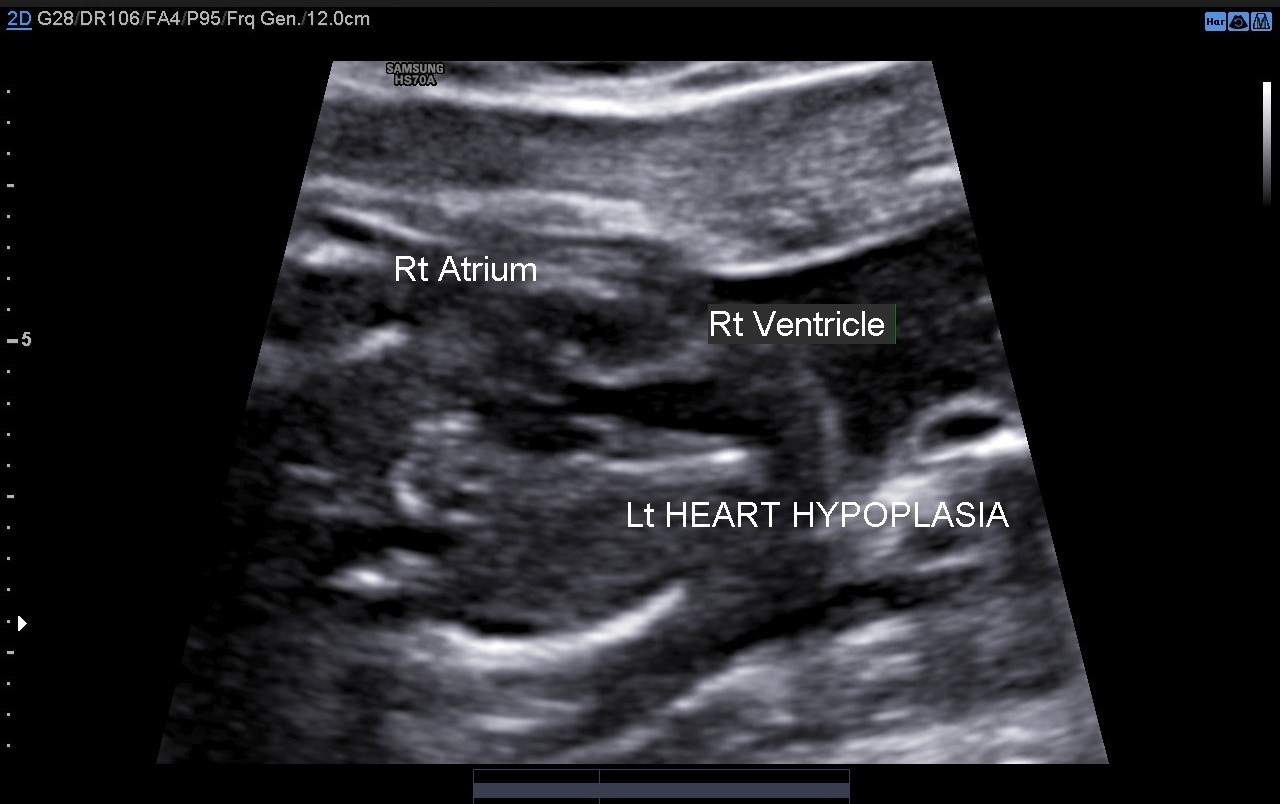
3. axial view of foetal heart shows abnormal 4 chamber view with hypoplastic left sided cardiac chambers suggestive of hypoplastic left heart syndrome / pulmonary isomerism; right sided cardiac chambers appear normal
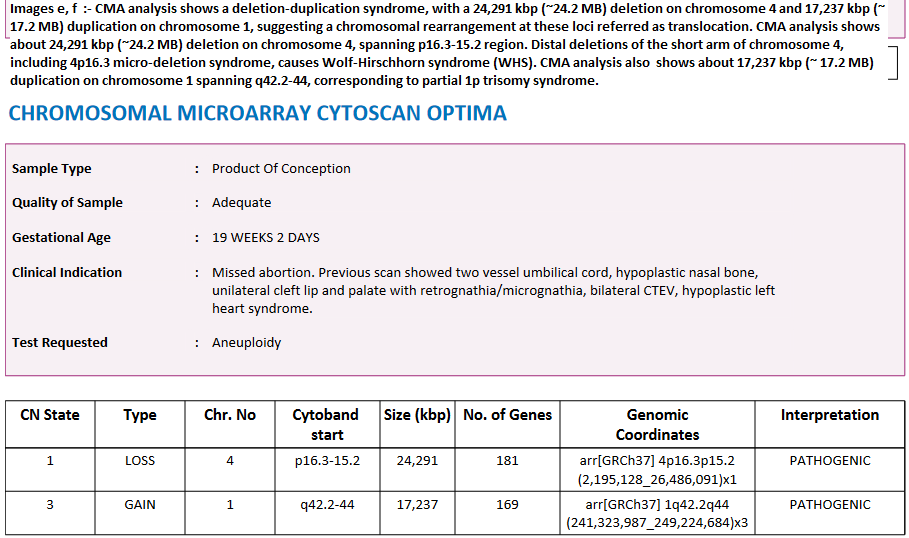
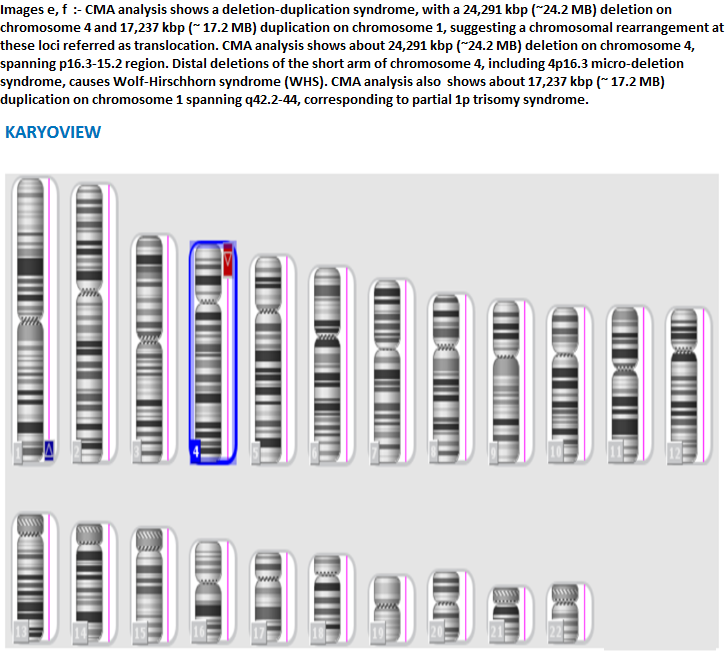
5. Chromosomal microarray analysis shows a deletion-duplication syndrome, with a 24,291 Kbp (~24.2 MB) deletion on chromosome 4 and 17,237 Kbp (~ 17.2 MB) duplication on chromosome 1, suggesting a chromosomal rearrangement at these loci referred as translocation. CMA analysis shows about 24,291 Kbp (~24.2 MB) deletion on chromosome 4, spanning p16.3-15.2 region. CMA analysis also shows about 17,237 Kbp (~ 17.2 MB) duplication on chromosome 1 spanning q42.2-44, corresponding to partial 1p trisomy syndrome.
CONCLUSION
The fetus in this case had many features of both syndromes.i. congenital anomalies associated with WHS, that were noted in this foetus are: Prenatal growth retardation (IUGR), facial deformities (Greek warrior helmet appearance: high forehead, prominent glabella, hypertelorism, high-arched eyebrows, protruding eyes and micrognathia), cardiac anomalies- pulmonary isomerism, abnormality of the external ear 1,2.ii. congenital anomalies associated with partial trisomy of chromosome 1, that were noted in this foetus are protruding forehead and micrognathia.
References:
1. Mozer Joaquim T, Paiva Grangeiro C, Gaona de Oliveira Gennaro F, Galvão Gomes A, Squire J, Martelli L. Partial Monosomy 4p and Trisomy 12q Due to a T(4;12)(p16.3;q24.31) Familial Translocation in Two Cousins. Mol Syndromol. 2019;10(5):264-71. doi:10.1159/000501923 - Pubmed
2. Rezai S. Wolf-Hirschhorn Syndrome (WHS), A Case Report and Review of Literature Submit Manuscript. JPNC. 2016;5(1):62-5. doi:10.15406/jpnc.2016.05.00170
3. Tartaglia E, Mastrantonio P, Costa D, Giugliano B, Porcellini A, Costagliola C. Trisomy 1q42-Qter Associated with Monosomy 6q27-Qter: A Case Report. Eur J Ophthalmol. 2010;21(3):315-9. doi:10.5301/ejo.2010.5796 - Pubmed